Journal of caring sciences.15(1) :9-19.
doi: 10.34172/jcs.026.33805
Original Article
Music Therapy for Pain and Anxiety control in Patients Undergoing Bone Marrow Biopsy and Aspiration: A Systematic review and Meta-analysis
Leila Sheikhnezhad Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 1 
Kosar Magbouli Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 2, *
Hamideh Zahedi Formal analysis, Methodology, Resources, Project administration, Validation, Writing – review & editing, 1
Hadi Hassankhani Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – review & editing, 3
Author information:
1Community Health Nursing Department, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz Iran
2Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
3Hematology and Oncology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Introduction:
Bone marrow biopsy and aspiration (BMBA) are invasive and painful procedures used to diagnose and monitor hematologic and non-hematologic disorders. Music therapy is known as a non- pharmacological approach to pain and anxiety management. However, there is an inconsistent findings regarding the effectiveness of music intervention on pain and anxiety control. We conducted a systematic review to synthesize and analyze the available evidence.
Methods:
In this systematic review, Google Scholar, PubMed, Web of Science, Cochrane, Scopus, and SID (Scientific Information Database) databases were searched until December 2023. Randomized controlled trials (RCTs) and quasi-experimental studies in English were eligible. Following screening, 4 studies (3 RCTs and 1 quasi-experimental study) were included. For meta-analysis, pain outcomes were analyzed using 3 RCTs, and anxiety outcomes were analyzed using all 4 studies (3 RCTs and 1 quasi-experimental study). Risk of bias was assessed using Cochrane tools (ROB-2 for RCTs, ROBINS-I for non-randomized studies). Meta-analysis was performed using RevMan 5.3, with standardized mean differences (SMDs) and 95% confidence intervals calculated for pain and anxiety outcomes.
Results:
Four studies (257 patients) were included in the review. Meta-analysis of the data showed listening to music during the bone marrow aspiration and biopsy may reduce pain (SMD -1.05, 95% CI -1.63 to -0.48; 3 trails), and anxiety (SMD -0.31, 95% CI -0.56 to -0.07). However, the certainty of evidence for both outcomes was assessed as very low according to the GRADE approach, due to serious risk of bias, inconsistency, and imprecision.
Conclusion:
Pain and anxiety are common during BMBA. While music therapy has been studied, the evidence is of very low certainty, so no strong clinical recommendations can be made. More high-quality, large-scale studies with standardized methods are needed to determine if music therapy is effective.
Keywords: Bone marrow examination, Music, Systematic review, Pain, Anxiety, Meta-analysis
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This study was self-funded by the authors and received no external financial support from any funding organization.
Introduction
Bone marrow biopsy) and aspiration (BMBA) are invasive methods to determine the characteristics of bone marrow cells and morphological, cytological, and histopathological evaluation.1 They are proven methods to evaluate bone marrow in wide spectrum of diseases such as hematologic malignancies, non-hematologic malignancies and tumor treatment response.2 Bone marrow biopsy (BMB) is considered a gold standard for confirming bone marrow involvement. This invasive method are performed for diagnosis, staging, and monitoring effectiveness of the treatment of blood disorders.2-4 Two sites are commonly used to access bone marrow in adults; the sternum and the iliac crest, a local anesthetic (3-5 ml lidocaine 2%) is injected into the subcutaneous tissue to anesthetize the biopsy site and reduce pain.5 The patient may also receive topical anesthetics (such as ethyl chloride spray or topical lidocaine þ prilocaine cream) and/or anxiolytics.6 Then, a needle is inserted through the skin into the bone and the patient may feel severe pain during this time. A small amount of bone marrow fluid is removed from the bone marrow with a syringe attached to the needle.7 Manual Jamshidi bone marrow biopsy needle with three bevels, six cutting edges, a pointed stylet, and a rounded handle have been used for BMBA since 2014.8
Patients who experience this procedure report a high level of pain despite the local anesthesia of the biopsy site.9 About 50-70% of patients describe this procedure as painful. Similarly, about 60-80% of patients experience a high level of anxiety before and during the procedure.10 This high level of anxiety increases the level of pain,3because anxiety disorders characterizes by symptoms such as functional and social fear, worry, panic attacks, avoidance behaviors which, in turn, can contribute to an increased perception of pain.11 The level of pain combined with factors such as social, physical, demographic, and psychological factors, and the disease process can be variable. About 30% of patients reported it as the worst pain in their life.8
Anticipated fear of a painful procedure can significantly amplify pain perception and induce anxiety, which can negatively impact patient quality of life.12 Anxiety before BMBA significantly affects the pain after it.13 Anxiety caused by bone marrow biopsy can be explained by the conditioned anxiety model. This means that anxiety is caused by conditioned stimuli that have already been associated with painful stimuli, and later even neutral stimuli cause anxiety and a learned response. This indicates the correlation between anxiety and pain in such a way that previous painful experiences cause more anxiety, which will automatically increase the feeling of pain.8
Two pharmacological or non-pharmacological methods are used to manage anxiety and pain.14 Music therapy is one of the methods used in this regard. Humans have used the healing potential of music to address a wide range of physical, emotional, social, and other concerns in every age and culture over the centuries. It can help reduce pain and stress levels by directing the patient’s attention from negative stimuli to pleasant and encouraging thoughts.15It has become a vital part of medical science in recent years. It is used to improve health and control the social, psychological, physiological, and emotional consequences of diseases.16,17 It can be used in the form of listening to live or pre-recorded music, or even playing an instrument, and writing music.16
Music therapy is a systematic intervention approach that can help patients improve their health and reduce anxiety and pain.18 Music reduces the level of anxiety of the person by affecting the self-esteem, mood, and motivation of the person. It also changes the mood by increasing the release of endorphins, subsequently relieves pain, and increases the quality of life.15,16 While music intervention appears to be a safe, convenient, and cost-effective method to reduce anxiety and related psychophysiological activity, existing systematic reviews report inconsistent findings regarding its efficacy, optimal implementation, and underlying mechanisms. For instance, a Cochrane review on music interventions for preoperative anxiety found that music listening may reduce anxiety, but noted considerable heterogeneity in outcomes and methodological limitations across studies.19 Similarly, a meta-analysis concluded that music could reduce anxiety and pain in patients undergoing biopsies, but highlighted variations related to music type, timing, and patient preference.20 Additionally, factors such as whether music is patient-selected or researcher-chosen, the genre of music, and the timing of intervention (before, during, or after the procedure) contribute to outcome variability.21 Given these inconsistencies and the absence of a clear consensus on the effectiveness of music intervention for pain and anxiety specifically during bone marrow biopsy and aspiration (BMBA), this study aims to systematically review and evaluate the effects of music interventions on procedure- related anxiety and pain among patients undergoing BMBA.
Research Highlights
What is the current knowledge?
-
Pain and anxiety are highly prevalent and distressing symptoms for patients undergoing bone marrow biopsy and aspiration (BMBA), despite the use of standard care.
-
Music therapy can be employed as a safe, feasible, and low-cost non-pharmacological intervention to manage pain and anxiety in patients.
What is new here?
-
This study suggest that music intervention may reduce both pain (SMD -1.05) and anxiety (SMD -0.31). However, the certainty of this evidence is very low due to serious risk of bias, inconsistency, and imprecision in the existing studies.
-
There is no established, evidence-based protocol integrating music therapy into routine BMBA care. It emphasizes the necessity for future high-quality RCTs with standardized music interventions, adequate blinding, and larger sample sizes to generate reliable evidence for clinical practice.
Materials and Methods
This systematic review was reported using the Cochrane Handbook for Systematic Reviews22 and according to the PRISMA statement and registered in the International Prospective Registry of Systematic Reviews (CRD42023468150: PROSPERO). In this study, PICO is determined in this way.
The research question of this systematic review was formulated based on the PICO framework as follows:
Population (P):
Adult patients (≥ 18 years) undergoing bone marrow biopsy and/or bone marrow aspiration for diagnostic or therapeutic purposes.
Intervention (I):
Music therapy interventions, including listening to live or prerecorded music, administered before, during, or after bone marrow biopsy and/or aspiration.
Comparison (C):
Standard care or routine clinical practice without music intervention.
Outcomes (O):
Pain intensity and anxiety levels, measured using validated assessment tools.
Search Strategy
A comprehensive search was performed in databases, PubMed, Web of Science, Cochrane, Scopus, Google Scholar as searching engine, and Persian databases (SID, MagIran, and Iran Medex), in December2023. The search strategy was designed to be reproducible and combined terms related to music therapy, pain, anxiety, bone marrow biopsy, and bone marrow aspiration. No time restrictions were applied. All randomized controlled trials and quasi-experimental studies comparing music therapy with no intervention or standard care were included in this study. Conference abstracts and studies that do not have relevant data were excluded from the study. Only studies published in English were included, although Persian databases were searched to identify any relevant English-language publications from those sources. The search was performed twice, once at the beginning of the study and once after it. The patients who underwent BMB and BMA were included in this study. The interventions included receiving any kind of music therapy. The control group did not receive any intervention. Anxiety and pain in patients undergoing bone marrow biopsy were the primary and secondary outcomes considered in this study.
Data Collection and Analysis
Selection of Studies
The study selection process employed a rigorous two-stage independent screening methodology to minimize bias. While a dual independent screening process was employed, formal statistical assessment of inter-rater agreement (e.g., via Cohen’s kappa) was not calculated. Endnote version 20 resource management software was used to manage the studies. After removing duplicates, two authors (L.Sh & K.M) independently reviewed the titles and abstracts of the extracted articles in terms of inclusion and exclusion criteria. Potentially relevant articles then proceeded to full-text review, which was likewise conducted independently by the same two reviewers. Any discrepancies regarding inclusion were first resolved through structured discussion between the two primary reviewers. If consensus could not be reached, a third reviewer (H.Z.) was consulted to make the final determination.
Data Extraction and Management
To extract the data, two authors (L.Sh & K.M) independently extracted the characteristics of the studies using the data extraction form based on the Cochrane Handbook.22 Discrepancies were resolved through discussion.
The extracted data included the first author’s name, study, country, and year of publication, study design, studied groups, intervention type, blinding type, follow-up period, and the number of participants (Table 1). The factors in each group are the health status of the participants, the pain and anxiety as primary and secondary outcomes, and the results. The extracted data were related to post-intervention values.
Risk of Bias Evaluation in the Included Studies
Two authors (H.Z. and L.Sh.) independently evaluated the risk of bias for all included studies using the criteria outlined in the Cochrane Handbook. The risk of bias in randomized controlled trials (RCTs) was assessed using the revised Cochrane Risk of Bias tool (ROB-2)24, examining the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, and selective outcome reporting. For non-randomized or quasi-experimental trials, the Risk Of Bias In Non-randomized Studies - of Interventions (ROBINS-I)25 tool was applied. Then, the reviewers were matched and any disagreements were resolved by consulting a third reviewer (H.H). The results of the risk of bias assessment for the RCT studies are summarized in Table 2 and the quasi-experimental study in Table 3.
Evaluating the Quality of Evidence Using the GRADE Approach
The quality of the evidence presented in the included studies in relation to the outcomes of the study was examined using the Grading of Recommendations Assessment, Development and Evaluation approach or the GRADE approach which includes five areas (Risk of bias, Imprecision, Inconsistency, Indirectness, and Publication bias).26 This evaluation was independently reviewed by two authors (H.Z & L.Sh) and any disagreement between the two authors was resolved through discussion with the third author (H.H). To examine the existence of clinical heterogeneity, all the trials included in the study were described and compared regarding the characteristics of the studied population and also the characteristics of the interventions presented to the study groups.
To examine the existence of statistical heterogeneity, the I2 statistic and its 95% confidence interval were used. In line with standard GRADE guidance, the certainty of the evidence for inconsistency was considered for downgrading if substantial heterogeneity was present, defined as I2 ≥ 50%.27 In evaluating the indirectness, the study population, intervention type, control group, and outcomes of the included studies were examined in terms of responding to the present review study question.28 In evaluating the imprecision, the included trials were examined in terms of the sufficient number of participants to calculate the effect estimate and the size of the confidence interval around the effect estimate.29 To calculate the quality of evidence for each of the examined outcomes, the quality of the evidence was reduced by one degree if there was a strong concern in any of the dimensions, and in the case of a very severe concern, the quality of the evidence was reduced by two degrees.
Effect Size Calculation
The pain and anxiety data were extracted for the control and intervention groups. To calculate the effects of the intervention on the continuous outcomes of the study in the trials, the mean changes and the standard deviation were calculated for each of the intervention and control groups in the pre-intervention and post-intervention phases. Standardized mean differences (SMDs) with 95% CI were reported if different scales were used in different studies to examine continuous outcomes.30
Table 1.
Characteristics of Studies
|
Author (s) /Location/ (year)
|
Study design
|
Study groups
|
Type of intervention/s
|
Type of blinding
|
Follow-up period
|
Number of participants in each group
|
Health status of participants
|
Main outcome/s
|
Results
|
| Ergin et al172022, Turkey |
RCT |
Group 1:
Treatment group
Group 2: Control group |
Classical Turkish music for 15 minutes before the procedure |
Open-label design |
Before and after BMBA |
Treatment: 34
Control: 34 |
Stable patients
undergoing BMBA |
Patients' pain and anxiety levels during BMBA |
Classical Turkish music prior to BMBA can reduce the pain and anxiety of patients |
| Özdemir et al13 2019, Turkey |
RCT |
Group 1:
Treatment group
Group 2: Control group |
Turkish classical music through headphones for thirty minutes during BMBA |
Open-label design |
Before and after BMAB |
Treatment:14
Control: 16 |
Stable patients
undergoing BMBA |
Effectiveness of Turkish classical music on pain intensity and anxiety levels during BMBA |
Classical Turkish music reduced the severity of pain and Anxiety levels increased significantly in the intervention group at the first follow-up compared to the second follow-up. |
| Shabanloei et al15 2010, Iran |
RCT- Semi-experimental |
Group 1:
Treatment group
Group 2: Control group |
Three songs that have a slow and steady rhythm During the BMBA |
Single blind |
Before and after BMAB |
Treatment: 50
Control: 50 |
Patients diagnosed with blood disorders and solid tumors |
Efficacy of music therapy on pain and anxiety control for patients undergoing bone marrow BMBA |
Participants who listened to music had lower level of anxiety and pain than those who did not listen to music |
| Danhauer et al232010, USA |
RCT |
Group 1:
Treatment group
Group 2: Control group |
Choosing from 8 music CDs with
various types of music (e.g., classical, harp, general instrumental, nature sounds, country,
gospel, and jazz) during BMB |
Open-label design |
post-procedure |
Treatment: 29
Control: 30 |
Patients with diagnosis of hematological malignancies |
The impact of music on perceived pain, anxiety, and satisfaction of patients undergoing BMB. |
There was no significant difference between the intervention group that received music and the control group without music in their anxiety and pain levels. |
Abbreviations: RCT: randomized control trials, BMAB: on marrow aspiration and biopsy.
Table 2.
Risk of bias of included studies (RCTs)
|
Bias
|
Authors' judgment
|
Support for judgment
|
|
Danhauer et al
(2010)
|
|
|
| Random sequence generation |
Unclear risk |
There is not enough information about the type of randomization |
| Allocation concealment |
High risk |
There is not enough information in this regard. |
| Blinding of participants and personnel |
High risk |
Open-label design |
| Blinding of outcome assessors |
High risk |
Open-label design |
| Incomplete outcome data |
Low risk |
4 participants in the intervention group were not analyzed due to missing data |
| Selective reporting |
Low risk |
Protocol is not available but it is clear that all pre-specified and expected outcomes of interest are reported |
|
Özdemir et al
13
(2019)
|
| Random sequence generation |
Low risk |
Participants were allocated into intervention and control groups, using computer random number generator. |
| Allocation concealment |
High risk |
There is not enough information in this regard. |
| Blinding of participants and personnel |
High risk |
Open-label design |
| Blinding of outcome assessors |
High risk |
Open-label design |
| Incomplete outcome data |
Low risk |
Two of 16 participants in the intervention group were excluded which reasons for missing data are not related to outcomes. |
| Selective reporting |
Low risk |
Protocol is not available and but pre-specified outcomes of interest to the review reported in the pre-specified way. |
|
Ergin et al
17
(2022)
|
| Random sequence generation |
Unclear risk |
Participants were allocated into intervention and control groups, using random sampling method. |
| Allocation concealment |
High risk |
There is not enough evidence in this regard. |
| Blinding of participants and personnel |
High risk |
Open-label design |
| Blinding of outcome assessors |
High risk |
Open-label design |
| Incomplete outcome data |
Low risk |
There is not any incomplete data. |
| Selective reporting |
Low risk |
Protocol is not available but it is clear that all pre-specified and expected outcomes of interest are reported. |
Table 3.
Risk of bias of included studies (Semi-experimental study)
|
Author
|
Shabanloei et al
15
(2010)
|
| Bias due to confounding |
Moderate |
| Bias in selection of participants |
Low |
| Bias in the classification of interventions |
Moderate |
| Bias due to deviations from intended interventions |
Low |
| Bias due to missing data |
Low |
| Bias in measurement of outcomes |
Low |
| Bias in selection of reported result |
Low |
| Overall |
Moderate |
Data Analysis
Data were analyzed using Review Manager 5.3 software to compare the study outcomes between the intervention and control groups when at least two trials were available. Statistical heterogeneity among the included studies was assessed using the I2 statistic.27
For the pain outcome, meta-analysis included data from three studies (n = 157). Heterogeneity was low (I2 = 25%), which is below the conventional threshold of 50% for substantial heterogeneity. Therefore, a fixed-effect model was used to calculate the pooled effect size.
For the anxiety outcome, meta-analysis included data from four studies (n = 257). Heterogeneity was substantial (I2 = 65%), exceeding the 50% threshold. Consequently, a random-effects model was used to calculate the pooled effect size, as this model accounts for between-study variance and provides a more conservative estimate when heterogeneity is present.
Result
The results of the literature search are summarized in the PRISMA diagram (Figure 1). A total of 356 studies were evaluated. After removing 176 duplicates, 180 records remained for title and abstract screening. 145 studies were excluded for not meeting inclusion criteria.After screening studies, 35 studies were reviewed and finally, 4 studies, including 3 RCT studies13,17,23and 1 quasi-experimental study,15 were included in the systematic review and meta-analysis.
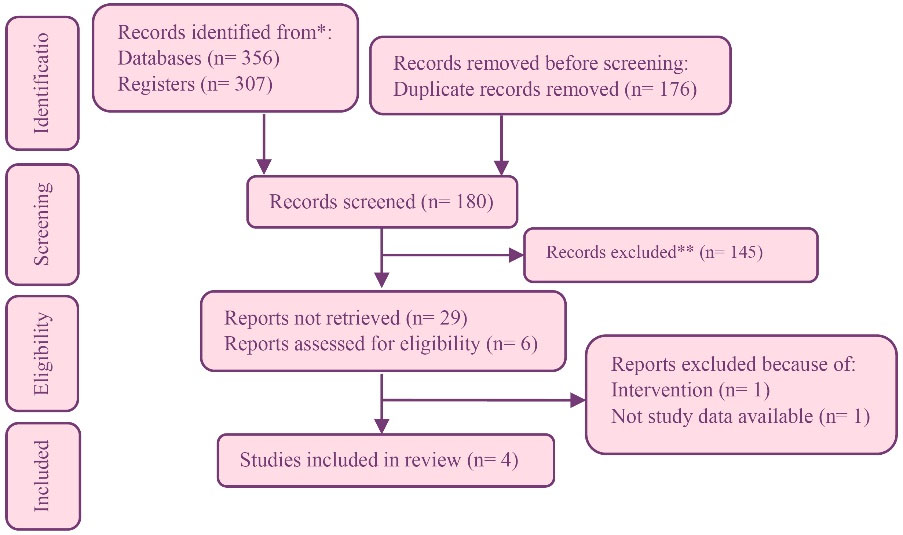
Figure 1.
Study flow diagram
.
Study flow diagram
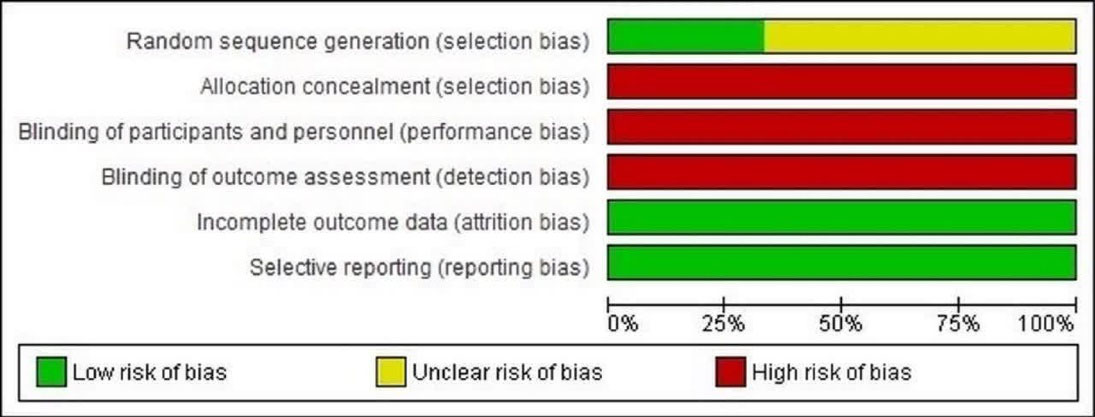
Figure 2.
Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies
.
Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies
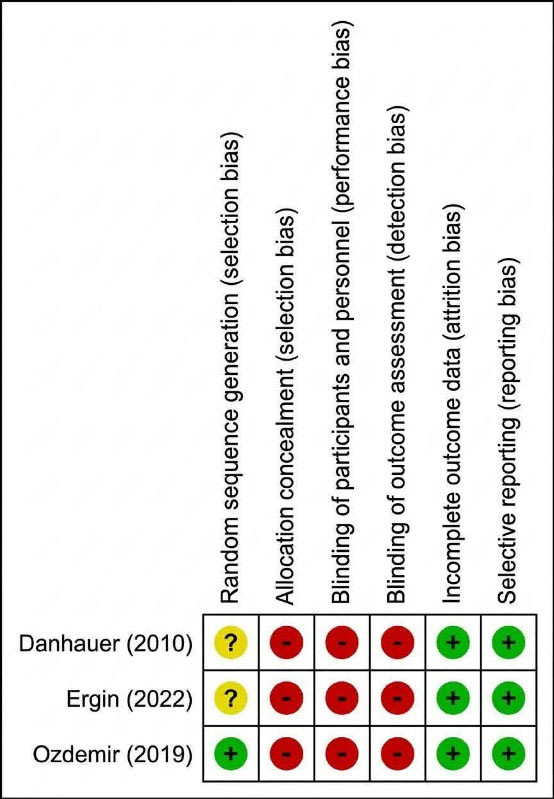
Figure 3.
Risk of bias summary: review authors’ judgments about each risk of bias item for each included study
.
Risk of bias summary: review authors’ judgments about each risk of bias item for each included study
Characteristics of Studies
Table 1 presents the characteristics of the included studies.
Included Studies
This study systematically reviews 3 RCTs and 1 quasi-experimental conducted on 257 patients who are candidates for BMBA All 4 articles were published between 2010 and 2022. All studies are written in English. In all 4 studies, the control group received routine treatments and the research group received music intervention to reduce pain and anxiety.
The type of music selected to reduce pain and anxiety during the procedure was different in the studies. In one study, the participants selected their favorite song from three CDs with similar songs.15 In Danhauer’s study, the participants of the research group selected their favorite music among the 8 CDs that were provided to them (classical, harp, general instrumental, nature sounds, country, gospel, and jazz.23 In two studies conducted in Turkey, Classical Turkish Music was used as an intervention.13,17
Results of the Meta-Analysis
In the meta-analysis of the data obtained from three studies conducted on 157 patients, it was shown that music therapy intervention compared to routine treatment may reduce patients’ pain (SMD, -1.05).
In the meta-analysis of the data obtained from four studies on 257 patients, results showed that providing music therapy intervention compared to routine treatment may reduce patients’ anxiety (SMD, -0.31).
Risk of Bias in the Included Studies
Figure 2, 3 shows the quality assessment of the RCTs included in this study. The overall risk of bias across the included studies was assessed as high (Figure 3), which substantially limits the certainty of the findings. Among the three randomized controlled trials included in the study, only one study was rated as low risk13, and two other studies were rated as uncertain risk17,23(Figure 4). Regarding the concealment of intervention allocation, blinding of participants and personnel, and study outcome assessors, all studies were rated as high risk. Regarding incomplete outcome information, attrition bias, and selective reporting bias, all studies were rated as low risk (Table 2)
In examining the risk of bias of the quasi-experimental trial included in this study, the overall risk of bias was considered moderate due to the presence of at least one moderate bias in the investigated subdomains. Accordingly, the desired study was at medium risk in terms of bias caused by confounders and in terms of bias caused by the classification of the desired intervention. It was at low risk regarding the bias caused by the selection of participants, the bias caused by the deviation from the interventions, the bias caused by missing data, the bias caused by the outcome measurement, and the selective reporting of the findings (Table 3).
Outcome Measurement
Pain
Three randomized controlled trials and one quasi-experimental trial compared pain levels in patients in the intervention (music therapy) and control (routine treatment) groups. All studies used the Visual Analog Scale (VAS) tool to assess pain. The results of three studies revealed that music therapy reduces the pain of bone marrow patients. Also, the results of one study did not reveal a significant difference between the control and intervention groups.23 All studies, except the study by Shabanlouei et al15 were included in the meta-analysis. Because this study did note provide separate pain scores for control and intervention groups. Data from three studies conducted on 157 patients revealed that music therapy may be more effective than routine treatment in reducing pain, but the level of evidence was uncertain (Figure 4).
The quality of evidence was reduced by three degrees and reached the level of very low certainty due to severe concern in the assessment of risk of bias and imprecision of included studies
Table 4.
Certainty of the evidence using the GRADE approach by outcomes
|
No of studies
|
Design
|
Risk of bias
|
Inconsistency
|
Indirectness
|
Imprecision
|
Publication bias
|
Music Therapy
|
Routine care
|
Pooled effect
Relative(95% CI)
|
Final judgment
|
|
Anxiety
|
| 4 |
RCT*
Semi-experimental |
very Serious |
Serious |
No serious |
serious |
No serious |
127 |
130 |
SMD 0.3 Lower (0.5 lower to 0.02 lower) |
⊕⊖⊖⊖
Very low |
|
Pain
|
| 3 |
RCT* |
Very Serious |
No serious |
No serious |
serious |
No serious |
77 |
80 |
SMD 1.05 Lower (1.6 lower to 0.4 lower) |
⊕⊖⊖⊖
Very low |
CI: confidence interval; RCT: randomized controlled trial; SMD: standardized mean difference.

Figure 4.
Music Intervention group versus Control group, outcome 1: Pain
(SMD -1.05, 95% CI -1.63 to -0.48; 3 trails, 157 patients, very low certainty)
.
Music Intervention group versus Control group, outcome 1: Pain
(SMD -1.05, 95% CI -1.63 to -0.48; 3 trails, 157 patients, very low certainty)

Figure 5.
Music Intervention group versus Control group, outcome 2: Anxiety
(SMD -0.31, 95% CI -0.56 to -0.07; 4 trails, 257 patients, very low certainty)
.
Music Intervention group versus Control group, outcome 2: Anxiety
(SMD -0.31, 95% CI -0.56 to -0.07; 4 trails, 257 patients, very low certainty)
Anxiety
Three studies15,17,23 employed the State-Trait Anxiety Inventory (STAI)31 to assess anxiety, while one study utilized the State Anxiety Inventory (SAI), The SAI is part of the STAI.13 Two studies demonstrated a significant reduction in anxiety levels among intervention15,17 groups. Additionally, one study did not find a significant difference between the intervention and control groups,23 and another study reported contradictory findings, a statistically significant increase in anxiety level was observed in the intervention group from the first to the second follow-up assessment.13 A meta-analysis of these four studies, encompassing 257 patients, suggested a potential beneficial effect of music therapy interventions on anxiety reduction compared to standard care, but the level of evidence was uncertain (Figure 5).
The quality of the evidence was reduced by three degrees and reached the level of very low certainty due to the existence of severe concerns in the assessment of the risk of bias, imprecision, and inconsistency of the included studies.
Justification for GRADE Assessment
The overall certainty of the evidence for both pain and anxiety outcomes was rated as very low. For pain, the certainty was downgraded by two levels due to a very serious risk of bias, as all three contributing RCTs had high risk in key domains such as blinding, and by one level for imprecision, owing to the small total sample size (n = 157) and a wide confidence interval around the effect estimate. For anxiety, the certainty was downgraded by one level each for risk of bias (due to high risk in blinding domains and a moderate risk of bias in the quasi-experimental study), inconsistency (indicated by substantial statistical heterogeneity, I2 = 65%, and contradictory findings among studies), and imprecision (as the confidence interval, while narrow, approached the line of no effect and the optimal information size was likely not met). (Table 4)
Discussion
In this systematic review and meta-analysis study, 3 RCT studies and 1 quasi-experimental study were included in the study to investigate the effect of music therapy on pain and anxiety in patients undergoing BMBA. The results were consistent with the possibility that music intervention during BMBA could contribute to reduced pain and anxiety in patients. However, further research is needed to confirm this effect. Pain and anxiety are the most common symptoms in patients undergoing invasive procedures.32-34 An increase in the level of pain mostly increases anxiety, and anxiety often increases the frequency or severity of pain.35 In this regard, a study by Hakimi et al showed that music therapy can effectively reduce postpartum pain and anxiety.36
In all 4 studies, the pain severity of 257 patients was measured using the VAS tool. Due to the subjective nature of pain, VAS is a valid tool to estimate the level of pain based on a person’s self-report.37 The results of a similar meta-analysis revealed that music intervention can reduce the pain caused by invasive biopsies.20 Compared to other interventions used to reduce pain, the results of a meta-analysis revealed that relaxation techniques may reduce some of the pain outcomes.38
Also, the results of a study by Brinie et al39 revealed strong support for distraction and hypnosis to reduce pain from needle-based procedures in children and adults. However, the quality of the available evidence was low.39 The results of a meta-analysis conducted to investigate the effect of distraction based on virtual reality on pain revealed that this type of distraction is highly effective in controlling burn pain. However, the results were inconsistent regarding the pain of needle-based procedures.40 A meta-analysis by Chow et al39 provided inconclusive evidence of the effect of immersive virtual reality (immersive VR) in reducing pain and anxiety associated with cancer treatment and diagnostic procedures, including bone marrow biopsy.41 A meta-analysis study reported that, contrary to expectations, neither music nor distraction was superior to routine care in managing procedural pain and anxiety in cancer patients. Some patients even found such interventions bothersome and had individual preferences for painful or anxiety-provoking procedures.42
Similar results have been reported in many RCTs that have measured the effect of music intervention as a non-pharmacological method to reduce the pain of painful procedures. For example, the results of reducing pain in broken noses,43 reducing the pain of patients with colorectal cancer,44 and reducing the pain of childbirth.45 Music may be an effective tool to reduce pain and anxiety and improve the mood of patients during active cancer treatment. However, methodological limitations of the studies conducted in this regard may reduce the evidence’s certainty.46 Understanding the nature of musical sound is critical to meeting the needs of each cancer patient and achieving the desired effect. One of the reasons for this is that music has an arousal-regulating effect. Passive listening to a single song seems to be the most effective type of music intervention.46
There is inconsistency in many studies investigating the effect of music intervention on pain reduction. Some researchers have attributed these contradictions to the lack of clarity about the cognitive mechanisms of action in the area of music therapy. Other reasons include small sample size, heterogeneity in the music type used as an intervention, methodological errors or the risk of low statistical power of studies included in previous RCT studies, the type of music selected, and passive or active listening to music. The uncertainty of the meta-analysis conducted about the effect of music on bone marrow biopsy pain is also debatable. Moreover, most studies do not pay attention to the importance of self-selected music and use the music selected by the research team.21 This issue may affect the results of the study. A meta-analysis study showed that music, especially when selected by the patient, can reduce pain after fracture surgeries.47 For example, no significant difference was observed between pain and anxiety scores in an RCT that investigated the effect of touch on pain and anxiety in patients undergoing bone marrow biopsy.48 The results also revealed that music is well received by patients and care providers since its implementation is easy and is considered a safe and cheap intervention.49
Some studies have reported anxiety as a major predictor of pain during biopsy.35 Thus, to reduce pain related to aspiration and predicted anxiety, pain prevention and management may need to be accompanied by pharmacological and non-pharmacological interventions.50 Patients with high anxiety levels experience higher levels of pain. Younger age, poor performance scores, and long procedures are other predictive factors for high levels of pain.51 A comparative study reported that a music intervention yielded anxiety reduction similar to midazolam injection in patients undergoing nerve block. This study, does not establish music as a clinical substitute for pharmacological anxiolytics. Rather, it highlights music’s potential as an adjunctive intervention.52
A study by Abbaszadeh et al3 investigated the effect of lavender scent on the anxiety of patients undergoing bone marrow biopsy and showed a significant difference between the two control and intervention groups in terms of anxiety scores (P < 0.05).3 The results of the meta-analysis by Song et al20 revealed that music reduced pre-biopsy systolic blood pressure, post-biopsy anxiety index score, post-biopsy diastolic blood pressure, and post-biopsy heart rate. Similarly, music was also more effective for post-biopsy pain control. However, the certainty of the evidence was moderate.20 Four included systematic reviews indicate that listening to music may have a positive impact on anxiety after surgery and invasive procedures.
These results are in line with those of four other systematic reviews on using music interventions to reduce anxiety in medical patients.19,53-55 Thus, we conclude that music interventions may be a suitable alternative to sedatives and anti-anxiety drugs to reduce preoperative anxiety. A study by Weisfeld et al56 compared the effects of various non-pharmacological methods in reducing pain and anxiety in patients undergoing medical and dental procedures. The results revealed that music is more effective in reducing anxiety compared to other non-pharmacological interventions such as massage, distraction, hypnosis, aromatherapy, acupuncture, social support, the sound of nature, and cognitive behavioral therapy (CBT).56 Thus, based on the results of the studies, music can be considered a safe alternative to reduce the pain and anxiety of patients undergoing BMBA.
Conclusion
Pain and anxiety are commonly reported symptoms among patients undergoing bone marrow biopsy and aspiration procedures. However, there is currently no approved protocol for oncology nurses that combines pharmacological and non-pharmacological methods to control them in patients. Although music therapy has been investigated as a non-pharmacological approach to reduce pain and anxiety during bone marrow biopsy and aspiration, the certainty of the current evidence is very low. Therefore, no firm clinical recommendations can be made. Future well-designed randomized controlled trials with larger sample sizes and standardized intervention protocols are required to clarify the potential role of music therapy in this clinical context.
Acknowledgements
With thanks to Hematology and Oncology Research Center and Student research committee of Tabriz University of Medical Sciences, Tabriz, Iran.
Competing Interests
The authors have no competing interest to declare.
Data Accessibility
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
Ethical approval for this study was obtained from the ethics committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1402.494).
GRADE Working Group grades of evidence
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
References
- Gyftopoulos S, Cardoso MDS, Wu JS, Subhas N, Chang CY. Bone Marrow Biopsies: Is CT, Fluoroscopy, or no Imaging Guidance the Most Cost-Effective Strategy? Acad Radiol 2024;31(7):2880–6. Is CT, Fluoroscopy, or no Imaging Guidance the Most Cost-Effective Strategy? Acad Radiol 2024; 31(7):Is CT, Fluoroscopy, or no Imaging Guidance the Most Cost-Effective Strategy? Acad Radiol 2024;31(7). doi: 10.1016/j.acra.2024.01.019 [Crossref] [ Google Scholar]
- Tomasian A, Jennings JW. Bone marrow aspiration and biopsy: techniques and practice implications. Skeletal Radiol 2022; 51(1):81-8. doi: 10.1007/s00256-021-03882-w [Crossref] [ Google Scholar]
- Abbaszadeh R, Tabari F, Asadpour A. The Effect of Lavender Aroma on Anxiety of Patients Having Bone Marrow Biopsy. Asian Pac J Cancer Prev 2020; 21(3):771-5. doi: 10.31557/apjcp.2020.21.3.771 [Crossref] [ Google Scholar]
- Draganski E, Deason T, Craig FE. Bone Marrow Aspiration and Biopsy Performed by RNs: A Review of Clinical Practice. Am J Nurs 2019; 119(9):47-53. doi: 10.1097/01.NAJ.0000580260.18537.ca [Crossref] [ Google Scholar]
- Islam A. Manual of bone marrow examination: Cambridge Scholars Publishing; 2020.
- Liptrott SJ, Botti S, Bonifazi F, Cioce M, De Cecco V, Pesce AR. Management of Pain and Anxiety during Bone Marrow Aspiration: An Italian National Survey. Pain Manag Nurs 2021; 22(3):349-55. doi: 10.1016/j.pmn.2020.09.005 [Crossref] [ Google Scholar]
- Hjortholm N, Jaddini E, Hałaburda K, Snarski E. Strategies of pain reduction during the bone marrow biopsy. Ann Hematol 2013; 92(2):145-9. doi: 10.1007/s00277-012-1641-9 [Crossref] [ Google Scholar]
- Escamilla-Gutiérrez ML, Guzmán-Saldaña RME, Galindo-Vázquez O, Vizcaino-Escobar AE. Psychological interventions for pain and anxiety management during bone marrow aspiration and biopsy. Mexican Journal of Medical Research ICSA 2023; 11(22):16-22. doi: 10.29057/mjmr.v11i22.10610 [Crossref] [ Google Scholar]
- Joshi S, Wader J, Kanethkar S. Bone marrow aspiration and bone marrow biopsy in hematological disorders. Biomedical and Pharmacology Journal 2020; 13(2):799-804. doi: 10.13005/bpj/1944 [Crossref] [ Google Scholar]
- Şahan S, Korkmaz E, Korkmaz S. The effect of music on comfort, pain, and anxiety in patients with bone marrow aspiration and biopsy in Turkey: a mixed-methods study. BMC Complement Med Ther 2024; 24(1):228. doi: 10.1186/s12906-024-04531-0 [Crossref] [ Google Scholar]
- Szuhany KL, Simon NM. Anxiety Disorders: A Review. Jama 2022; 328(24):2431-45. doi: 10.1001/jama.2022.22744 [Crossref] [ Google Scholar]
- Cerchione C, Martinelli G, Picardi M, Pugliese N, Nappi D, Casoria A. Combined Oral Fentanyl Citrate and Midazolam as Premedication for Bone Marrow Aspiration and Biopsy in Patients with Hematological Malignancies: A Randomized, Controlled and Patient-Blinded Clinical Trial. J Clin Med 2020; 9(2):395. doi: 10.3390/jcm9020395 [Crossref] [ Google Scholar]
- Özdemir Ü, Taşcı S, Yıldızhan E, Aslan S, Eser B. The Effect of Classical Turkish Music on Pain Severity and Anxiety Levels in Patients Undergoing Bone Marrow Aspiration and Biopsy. Pain Manag Nurs 2019; 20(1):82-7. doi: 10.1016/j.pmn.2018.04.009 [Crossref] [ Google Scholar]
- Tola YO, Chow KM, Liang W. Effects of non-pharmacological interventions on preoperative anxiety and postoperative pain in patients undergoing breast cancer surgery: A systematic review. J Clin Nurs 2021; 30(23-24):3369-84. doi: 10.1111/jocn.15827 [Crossref] [ Google Scholar]
- Shabanloei R, Golchin M, Esfahani A, Dolatkhah R, Rasoulian M. Effects of music therapy on pain and anxiety in patients undergoing bone marrow biopsy and aspiration. Aorn j 2010; 91(6):746-51. doi: 10.1016/j.aorn.2010.04.001 [Crossref] [ Google Scholar]
- Kalel MJ, Shawq AH. Music Medicine Intervention–Based Program for Reducing Pain and Anxiety of Children Undergoing Bone Marrow Aspiration and Lumber Puncture Procedures. Pakistan Heart Journal 2023; 56(2):407-13. [ Google Scholar]
- Ergin E, Kahriman F, Coşan Ay H, Çınar Yücel Ş. Effect of classical Turkish music on Pain and anxiety of patients undergoing bone marrow aspiration and biopsy: a Randomized Controlled Clinical Trial. Journal of Holistic Nursing And Midwifery 2022; 32(3):227-33. doi: 10.32598/jhnm.32.3.2259 [Crossref] [ Google Scholar]
- Ting B, Tsai CL, Hsu WT, Shen ML, Tseng PT, Chen DT. Music Intervention for Pain Control in the Pediatric Population: A Systematic Review and Meta-Analysis. J Clin Med 2022; 11(4):991. doi: 10.3390/jcm11040991 [Crossref] [ Google Scholar]
- Bradt J, Dileo C, Shim M. Music interventions for preoperative anxiety. Cochrane Database Syst Rev 2013; 2013(6):Cd006908. doi: 10.1002/14651858.CD006908.pub2 [Crossref] [ Google Scholar]
- Song M, Li N, Zhang X, Shang Y, Yan L, Chu J. Music for reducing the anxiety and pain of patients undergoing a biopsy: A meta-analysis. J Adv Nurs 2018; 74(5):1016-29. doi: 10.1111/jan.13509 [Crossref] [ Google Scholar]
- Howlin C, Rooney B. The Cognitive Mechanisms in Music Listening Interventions for Pain: A Scoping Review. J Music Ther 2020; 57(2):127-67. doi: 10.1093/jmt/thaa003 [Crossref] [ Google Scholar]
- Chandler J, Cumpston M, Li T, Page MJ, Welch V. Cochrane handbook for systematic reviews of interventions. Hoboken: Wiley. 2019.
- Danhauer SC, Vishnevsky T, Campbell CR, McCoy TP, Tooze JA, Kanipe KN. Music for patients with hematological malignancies undergoing bone marrow biopsy: a randomized controlled study of anxiety, perceived pain, and patient satisfaction. J Soc Integr Oncol 2010; 8(4):140-7. [ Google Scholar]
- Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Assessing risk of bias in a randomized trial. Cochrane Handbook for Systematic Reviews of Interventions2019. p. 205–28.
- Jüni P, Loke Y, Pigott T, Ramsay C, Regidor D, Rothstein H. Risk of bias in non- randomized studies of interventions (ROBINS-I): detailed guidance. Br Med J 2016; 355:i4919. [ Google Scholar]
- Kirmayr M, Quilodrán C, Valente B, Loezar C, Garegnani L, Franco JVA. The GRADE approach, Part 1: how to assess the certainty of the evidence. Medwave 2021; 21(2):e8109. doi: 10.5867/medwave.2021.02.8109 [Crossref] [ Google Scholar]
- Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et alGRADE guidelines: 7Rating the quality of evidence--inconsistency. J Clin Epidemiol 2011; 64(12):1294-302. doi: 10.1016/j.jclinepi.2011.03.017 [Crossref] [ Google Scholar]
- Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et alGRADE guidelines: 8Rating the quality of evidence--indirectness. J Clin Epidemiol 2011; 64(12):1303-10. doi: 10.1016/j.jclinepi.2011.04.014 [Crossref] [ Google Scholar]
- Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D. Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et alGRADE guidelines 6Rating the quality of evidence--imprecision. J Clin Epidemiol 2011; 64(12):1283-93. doi: 10.1016/j.jclinepi.2011.01.012 [Crossref] [ Google Scholar]
- Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making 2013; 33(5):607-17. doi: 10.1177/0272989x12458724 [Crossref] [ Google Scholar]
- Spielberger CD, Gonzalez-Reigosa F, Martinez-Urrutia A, Natalicio LF, Natalicio DS. The state- trait anxiety inventory. Revista Interamericana de Psicologia/Interamerican journal of psychology 1971;5(3 & 4).
- Azak M, Aksucu G, Çağlar S. The Effect of Parental Presence on Pain Levels of Children During Invasive Procedures: A Systematic Review. Pain Manag Nurs 2022; 23(5):682-8. doi: 10.1016/j.pmn.2022.03.011 [Crossref] [ Google Scholar]
- Gheshlaghi PA, Farahani ZB, Anboohi SZ, Nasiri M, Ziapour A, Garosi VH. Effect of family presence on pain and anxiety levels among patients during invasive nursing procedures in an emergency department at a public hospital in Western Iran. Afr J Emerg Med 2021; 11(1):31-6. doi: 10.1016/j.afjem.2020.11.003 [Crossref] [ Google Scholar]
- Ganesan P, Manjini KJ, Bathala Vedagiri SC. Effect of Music on Pain, Anxiety and Physiological Parameters among Postoperative Sternotomy Patients: A Randomized Controlled Trial. J Caring Sci 2022; 11(3):139-47. doi: 10.34172/jcs.2022.18 [Crossref] [ Google Scholar]
- Kavak Akelma F, Altınsoy S, Arslan MT, Ergil J. Effect of favorite music on postoperative anxiety and pain. Anaesthesist 2020; 69(3):198-204. doi: 10.1007/s00101-020-00731-8 [Crossref] [ Google Scholar]
- Hakimi S, Hajizadeh K, Hasanzade R, Ranjbar M. A Systematic Review and Meta-analysis of the Effects of Music Therapy on Postpartum Anxiety and Pain Levels. J Caring Sci 2021; 10(4):230-7. doi: 10.34172/jcs.2021.033 [Crossref] [ Google Scholar]
- Weigl K, Forstner T. Design of Paper-Based Visual Analogue Scale Items. Educ Psychol Meas 2021; 81(3):595-611. doi: 10.1177/0013164420952118 [Crossref] [ Google Scholar]
- Vambheim SM, Kyllo TM, Hegland S, Bystad M. Relaxation techniques as an intervention for chronic pain: A systematic review of randomized controlled trials. Heliyon 2021; 7(8):e07837. doi: 10.1016/j.heliyon.2021.e07837 [Crossref] [ Google Scholar]
- Birnie KA, Noel M, Parker JA, Chambers CT, Uman LS, Kisely SR. Systematic review and meta-analysis of distraction and hypnosis for needle-related pain and distress in children and adolescents. J Pediatr Psychol 2014; 39(8):783-808. doi: 10.1093/jpepsy/jsu029 [Crossref] [ Google Scholar]
- Malloy KM, Milling LS. The effectiveness of virtual reality distraction for pain reduction: a systematic review. Clin Psychol Rev 2010; 30(8):1011-8. doi: 10.1016/j.cpr.2010.07.001 [Crossref] [ Google Scholar]
- Chow H, Hon J, Chua W, Chuan A. Effect of Virtual Reality Therapy in Reducing Pain and Anxiety for Cancer-Related Medical Procedures: A Systematic Narrative Review. J Pain Symptom Manage 2021; 61(2):384-94. doi: 10.1016/j.jpainsymman.2020.08.016 [Crossref] [ Google Scholar]
- Kwekkeboom KL. Music versus distraction for procedural pain and anxiety in patients with cancer. Oncol Nurs Forum 2003; 30(3):433-40. doi: 10.1188/03.Onf.433-440 [Crossref] [ Google Scholar]
- Ortega A, Gauna F, Munoz D, Oberreuter G, Breinbauer HA, Carrasco L. Music Therapy for Pain and Anxiety Management in Nasal Bone Fracture Reduction: Randomized Controlled Clinical Trial. Otolaryngol Head Neck Surg 2019; 161(4):613-9. doi: 10.1177/0194599819856604 [Crossref] [ Google Scholar]
- Huang E, Huang J. Music Therapy: A Noninvasive Treatment to Reduce Anxiety and Pain of Colorectal Cancer Patients-A Systemic Literature Review. Medicina (Kaunas) 2023; 59(3):482. doi: 10.3390/medicina59030482 [Crossref] [ Google Scholar]
- Santiváñez-Acosta R, Tapia-López ELN, Santero M. Music Therapy in Pain and Anxiety Management during Labor: A Systematic Review and Meta-Analysis. Medicina (Kaunas) 2020; 56(10):526. doi: 10.3390/medicina56100526 [Crossref] [ Google Scholar]
- Bro ML, Jespersen KV, Hansen JB, Vuust P, Abildgaard N, Gram J. Kind of blue: A systematic review and meta-analysis of music interventions in cancer treatment. Psychooncology 2018; 27(2):386-400. doi: 10.1002/pon.4470 [Crossref] [ Google Scholar]
- Lin CL, Hwang SL, Jiang P, Hsiung NH. Effect of Music Therapy on Pain After Orthopedic Surgery-A Systematic Review and Meta-Analysis. Pain Pract 2020; 20(4):422-36. doi: 10.1111/papr.12864 [Crossref] [ Google Scholar]
- Dhawan N, Schaal A, Pushee JR, Broglio K. The effect of touch on pain, anxiety, and the patient experience during bone marrow biopsies. American Society of Clinical Oncology; 2023. 10.1200/JCO.2023.41.16_suppl.e24131
- Schandert LC, Affronti ML, Prince MS, Schneider SM. Music Intervention: Nonpharmacologic Method to Reduce Pain and Anxiety in Adult Patients Undergoing Bone Marrow Procedures. Clin J Oncol Nurs 2021; 25(3):314-20. doi: 10.1188/21.Cjon.314-320 [Crossref] [ Google Scholar]
- Gendron N, Zia Chahabi S, Poenou G, Rivet N, Belleville-Rolland T, Lemaire P. Pain assessment and factors influencing pain during bone marrow aspiration: A prospective study. PLoS One 2019; 14(8):e0221534. doi: 10.1371/journal.pone.0221534 [Crossref] [ Google Scholar]
- Tanasale B, Kits J, Kluin PM, Trip A, Kluin-Nelemans HC. Pain and anxiety during bone marrow biopsy. Pain Manag Nurs 2013; 14(4):310-7. doi: 10.1016/j.pmn.2011.06.007 [Crossref] [ Google Scholar]
- Graff V, Cai L, Badiola I, Elkassabany NM. Music versus midazolam during preoperative nerve block placements: a prospective randomized controlled study. Reg Anesth Pain Med 2019. 10.1136/rapm-2018-100251
- Pittman S, Kridli S. Music intervention and preoperative anxiety: an integrative review. Int Nurs Rev 2011; 58(2):157-63. doi: 10.1111/j.1466-7657.2011.00888.x [Crossref] [ Google Scholar]
- Gillen E, Biley F, Allen D. Effects of music listening on adult patients’ pre-procedural state anxiety in hospital. JBI Libr Syst Rev 2008; 6(17):686-732. doi: 10.11124/01938924-200806170-00001 [Crossref] [ Google Scholar]
- Nilsson U. The anxiety- and pain-reducing effects of music interventions: a systematic review. Aorn j 2008; 87(4):780-807. doi: 10.1016/j.aorn.2007.09.013 [Crossref] [ Google Scholar]
- Weisfeld CC, Turner JA, Dunleavy K, Ko A, Bowen JI, Roelk B. Dealing with Anxious Patients: A Systematic Review of the Literature on Nonpharmaceutical Interventions to Reduce Anxiety in Patients Undergoing Medical or Dental Procedures. J Altern Complement Med 2021; 27(9):717-26. doi: 10.1089/acm.2020.0504 [Crossref] [ Google Scholar]